
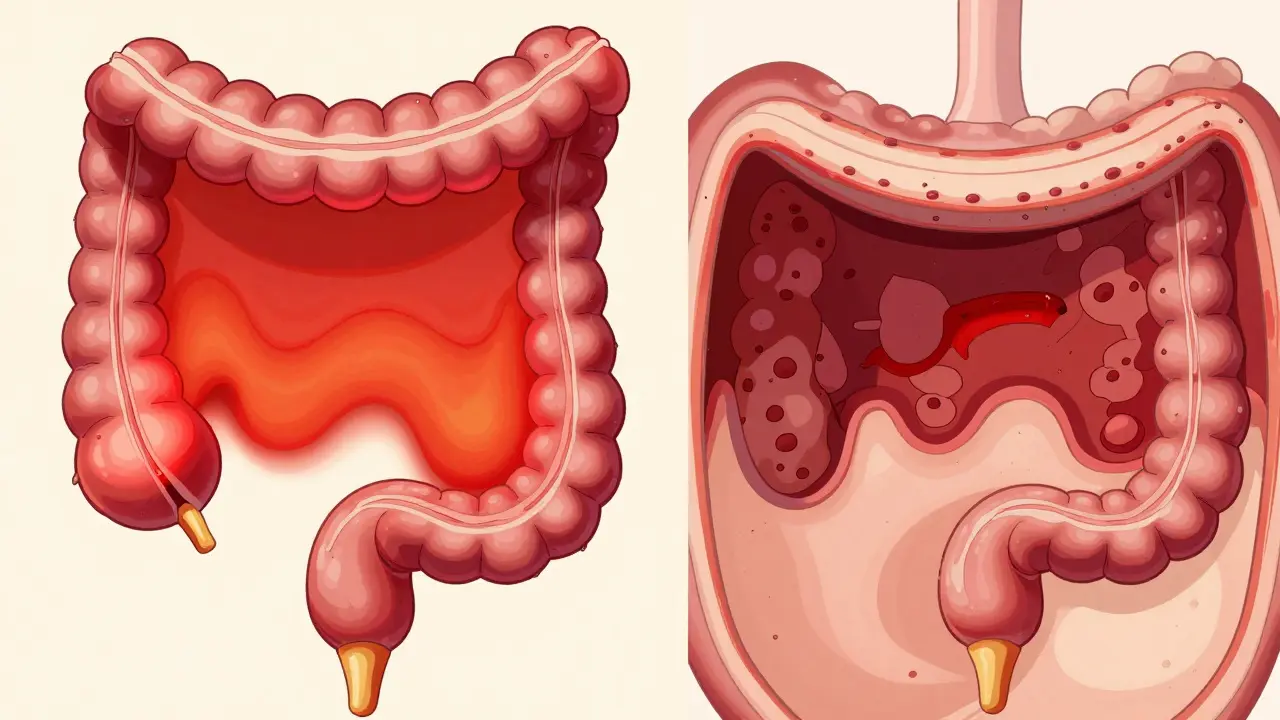
Ulcerative Colitis is a chronic inflammatory bowel disease (IBD) that causes inflammation and ulcers in the innermost lining of the colon and rectum. Unlike some other digestive issues, it follows a continuous pattern, meaning it starts at the rectum and spreads upward without skipping any patches of healthy tissue. It's an autoimmune struggle where the body's defense system targets the very walls meant to absorb water and nutrients from your food.
How Inflammation Maps Out in Your Colon
Not every case of UC looks the same. Depending on how far the inflammation travels up your colon, the symptoms and the impact on your day-to-day life can vary wildly. Doctors generally group these into five main types:
- Ulcerative Proctitis: This is the mildest form, where inflammation is confined strictly to the rectum (usually less than 6 inches). You might notice rectal bleeding, but you won't typically feel systemic illness.
- Proctosigmoiditis: The inflammation moves past the rectum into the sigmoid colon.
- Left-Sided Colitis: Here, the inflammation reaches the splenic flexure near your spleen. People with this type often feel significant cramping and pain specifically on the left side of their abdomen.
- Pancolitis: This is the most severe version. The entire colon is inflamed, which often leads to weight loss, loss of appetite, and severe bloody diarrhea.
- Rectal-Sparing UC: A rare version where the colon is inflamed, but the rectum remains strangely untouched.
The severity often dictates the frequency of bathroom trips. If the disease is limited to the rectum, your stool might actually seem normal or dry, though it's often accompanied by mucus and blood. However, once it moves higher up the large intestine, things get tougher. It's not uncommon for someone with extensive inflammation to deal with more than 10 bowel movements a day.
Spotting the Signs: Beyond the Bathroom
We often talk about the "classic" symptoms-bloody diarrhea, urgency, and that frustrating feeling called tenesmus, where you feel like you need to go even when your bowels are empty. But UC doesn't always stay in the gut. About 25% to 40% of people experience extra-intestinal symptoms. This means your immune system might cause joint swelling, skin lumps, or even eye irritation.
Flare-ups can be sneakily gradual, starting with mild lower abdomen cramps and a bit of blood in the stool. Other times, they hit like a freight train: violent diarrhea, high fever, and intense abdominal pain that makes it impossible to sleep. Because these flares can last for weeks and return without warning, the goal isn't just treating the flare-it's stopping the next one before it starts.
UC vs. Crohn's Disease: What's the Difference?
People often confuse Ulcerative Colitis with
Crohn's Disease, but they are biologically different. If you think of the digestive tract as a pipe, UC only paints the inside of the very end of that pipe (the colon and rectum). It never goes deeper than the inner lining.
Crohn's, on the other hand, is a "deep dive." It can cause inflammation through every single layer of the intestinal wall and can pop up anywhere from your mouth to your anus. While UC is a continuous wave of inflammation, Crohn's often presents as "skip lesions," where a patch of diseased tissue is followed by a patch of perfectly healthy tissue. Understanding this distinction is vital because it changes how surgeons and gastroenterologists approach treatment.
| Feature | Ulcerative Colitis | Crohn's Disease |
|---|---|---|
| Location | Colon and Rectum only | Anywhere in GI tract |
| Inflammation Depth | Inner lining only (Mucosal) | All layers (Transmural) |
| Pattern | Continuous | Patchy (Skip Lesions) |
| Rectal Involvement | Almost always involved | Variable |
Strategies for Achieving and Maintaining Remission
Remission isn't just about the absence of blood; it's about getting your life back. The medical approach usually follows a "step-up" strategy, starting with the gentlest options and moving toward more aggressive therapies if the disease doesn't budge.
For mild to moderate cases, the first line of defense is usually
5-aminosalicylates (also known as 5-ASAs), which are anti-inflammatory medications designed to soothe the lining of the colon. If those aren't enough, doctors move to immunomodulators, such as azathioprine, which help dampen the overactive immune response.
For those with severe or refractory disease,
Biologic Therapies have been a game-changer. These are advanced drugs that target specific proteins in the immune system to stop inflammation at the molecular level. In extreme cases where medication fails or the risk of colon cancer becomes too high-especially in pancolitis-a colectomy (surgical removal of the colon) may be the only way to stop the disease.
The Role of Triggers and Lifestyle
Here is a crucial point that often gets lost: food and stress do not cause Ulcerative Colitis. You didn't do anything to trigger the onset of this disease. However, while they aren't the cause, they are frequent triggers.
A high-stress month at work or a specific food sensitivity can push a stable system into a flare. During a flare, your appetite may vanish, and you might lose weight rapidly. This is where a personalized approach is key. Some find that low-residue diets help reduce the number of bowel movements, while others find specific dairy or spicy foods act as catalysts for pain. The trick is tracking your symptoms to find your personal "danger foods."

Long-Term Monitoring and Safety
Because UC causes chronic inflammation, the cells in the colon lining turn over more quickly than they should. Over many years, this increases the risk of developing dysplasia or colon cancer. This is why regular colonoscopies aren't optional-they are a vital safety net. By monitoring the health of the tissue, doctors can catch precancerous changes early. This is particularly critical for those with pancolitis, as the wider area of inflammation leads to a higher statistical risk compared to someone with only proctitis.
Can I ever truly cure Ulcerative Colitis?
There is currently no known cure for UC, but the goal is "clinical remission." This is a state where the inflammation is gone, symptoms disappear, and you can lead a completely active life. While the condition remains in your system, it can stay dormant for years with the right medication and monitoring.
Will I eventually need surgery?
Not necessarily. Many people manage their symptoms effectively for their entire lives using 5-ASAs or biologics. Surgery (colectomy) is typically reserved for severe cases where medication no longer works, or if there are complications like toxic megacolon or a high risk of malignancy.
Does a gluten-free diet help with UC?
Gluten-free diets are specifically for Celiac disease, not UC. However, some UC patients find that avoiding gluten or processed grains reduces their symptoms during a flare. Since triggers are individual, it's best to experiment with a food diary rather than following a generic diet.
Why do I feel joint pain when I have a colon issue?
This is known as an extra-intestinal manifestation. Because UC is an autoimmune disease, the inflammation isn't always limited to the gut. The same immune response attacking your colon can also target the joints, skin, or eyes, leading to arthritis or skin ulcers.
How often should I get a colonoscopy?
The frequency depends on the extent of your disease. Those with pancolitis generally require more frequent screenings than those with proctitis due to a higher risk of dysplasia. Your gastroenterologist will set a schedule based on your specific inflammation history.
Next Steps for Recovery
If you are currently in a flare, your first priority is stabilizing the inflammation. Focus on hydration and a bland diet to avoid irritating the bowel further. If you are in remission, the focus shifts to maintenance. Don't stop your medication just because you feel great-that's often when the immune system starts gearing up for another attack.
For those feeling overwhelmed, consider a support group. Dealing with the urgency and unpredictability of UC can be isolating, and speaking with others who understand the "bathroom anxiety" can be just as healing as the medication itself.

11 Comments
Jamar Taylor
Keep pushing forward everyone! You've got the strength to beat this and get your life back! 🚀
dwight koyner
It is imperative to emphasize that the transition from 5-ASAs to biologics should be managed closely by a gastroenterologist to ensure the most effective titration. Many patients find that combined therapy, rather than a strict step-up approach, yields faster results in achieving mucosal healing. Additionally, incorporating a low-FODMAP diet during active flares may alleviate some of the bloating and gas associated with these conditions, although it is not a treatment for the inflammation itself. Regular monitoring of C-reactive protein (CRP) and fecal calprotectin levels provides an objective measure of inflammation that symptoms alone cannot convey. This allows for preemptive adjustments to medication before a full-blown flare occurs. Ensuring a comprehensive support system including a registered dietitian specializing in IBD can significantly improve quality of life outcomes. One should also remain vigilant regarding the side effects of immunomodulators, specifically the increased susceptibility to opportunistic infections. Proper vaccination schedules are crucial and should be discussed before starting these therapies. The psychological toll of chronic illness often manifests as anxiety or depression, making cognitive behavioral therapy a valuable adjunct to medical treatment. Ultimately, the goal is not just clinical remission but deep histological remission where the tissue looks normal under a microscope. This reduces the long-term risk of colitis-associated colorectal cancer significantly. Stay diligent with your screenings.
Ethan Davis
Sure, just trust the 'big pharma' drugs and their 'step-up' plan. Funny how they never mention the stuff in the water causing this in the first place
Just another way to keep us hooked on biologics for life while they ignore the real culprits
Stephen Luce
I totally get that feeling of isolation. It's so hard when people don't understand why you have to map out every single bathroom in a building before you even enter it.
Jitesh Mohun
stop blaming food for everything just follow the meds and get your life back dont let the pain win
Jay Vernon
So glad to see a guide like this! Helpful stuff for everyone! 😊✨
shelley wales
Remember that you are not alone in this journey. Even on the hardest days, there is a community here supporting you and cheering you on toward remission. We can all get through this together!
Timothy Burroughs
you people just lack the discipline to cleanse your systems properly
back in a real country we have standards for health and dont just rely on these expensive chemicals from labs
Srikanth Makineni
biologics are the only thing that actually worked for me
Dhriti Chhabra
I believe it is of utmost importance to maintain a harmonious balance between medical intervention and mental well-being to facilitate a full recovery.
Brady Davis
Oh wow, a 'guide' to having your insides turn into a volcano. Truly the most thrilling read of my entire life. I'm just vibrating with excitement over the prospect of more colonoscopies!